Post-Acute Care's Dirty Secret: Manual RCM Is Costing You Millions


Here's the brutal truth: while everyone obsesses over value-based care strategies and population health management, post-acute care providers are hemorrhaging money through archaic revenue cycle processes that belong in the 1990s.
I've witnessed firsthand how manual RCM processes are killing post-acute facilities. These organizations spend more time fighting with payers over $500 underpayments than they do optimizing care for patients who need it most.
We're talking about $60 billion in Medicare post-acute spending annually, yet most facilities still use fax machines and Excel spreadsheets to manage their financial lifeline. This isn't just inefficient - it's financial malpractice.
The Value-Based Care Paradox: Why PAC Providers Are Drowning
Value-based contracts demand precision, yet post-acute care operates with revenue cycle systems designed for chaos. The contradiction is staggering:
- The Promise: Reduce costs, improve outcomes, share risk
- The Reality: Manual eligibility checks that take 45 minutes per patient
- The Irony: You're responsible for total cost of care but can't efficiently manage your own billing
I recently spoke with a post-acute administrator who told me their team spends 6 hours daily just sorting through referral faxes. Six hours. In 2025. While hospitals are discharging patients faster than ever (average length of stay before PAC discharge has increased by a full day since 2019 due to processing delays alone).
This isn't sustainable. It's not even sane.
Why Most RCM "Solutions" Are Snake Oil
Let me be blunt about the vendor landscape: most RCM solutions for post-acute care are half-baked attempts to retrofit acute care systems for different needs. They promise everything, deliver confusion, and leave you more frustrated than when you started.
The typical implementation goes like this:
- Vendor promises seamless integration
- Six months later, you're still trying to get basic eligibility verification working
- Your staff spends more time managing the "solution" than doing actual work
- You're told the next update will fix everything
- Repeat indefinitely
I've seen facilities spend $200,000+ on RCM systems that made their operations worse. The common thread? They focused on features instead of outcomes.
The RCM Automation Revolution: What Actually Works
Real RCM automation in post-acute care isn't about flashy dashboards or AI buzzwords. It's about eliminating the mind-numbing tasks that make competent staff want to quit.
Here's what genuine automation looks like:
- Referral Intake That Actually Works: Instead of staff printing faxes and manually entering data, AI systems read referrals, extract patient information, verify insurance eligibility, and create complete patient records. In under 30 seconds.
- Authorization That Doesn't Drive People Insane: The system predicts which services need authorization based on diagnosis, payer type, and historical data. It gathers required documentation automatically and submits requests without human intervention.
- Documentation That Writes Itself: As clinical staff provide care, the system captures billable activities, matches them to appropriate codes, and ensures medical necessity documentation is complete. No more midnight documentation marathons.
The Numbers Don't Lie
Let me share some actual numbers from facilities I've worked with:
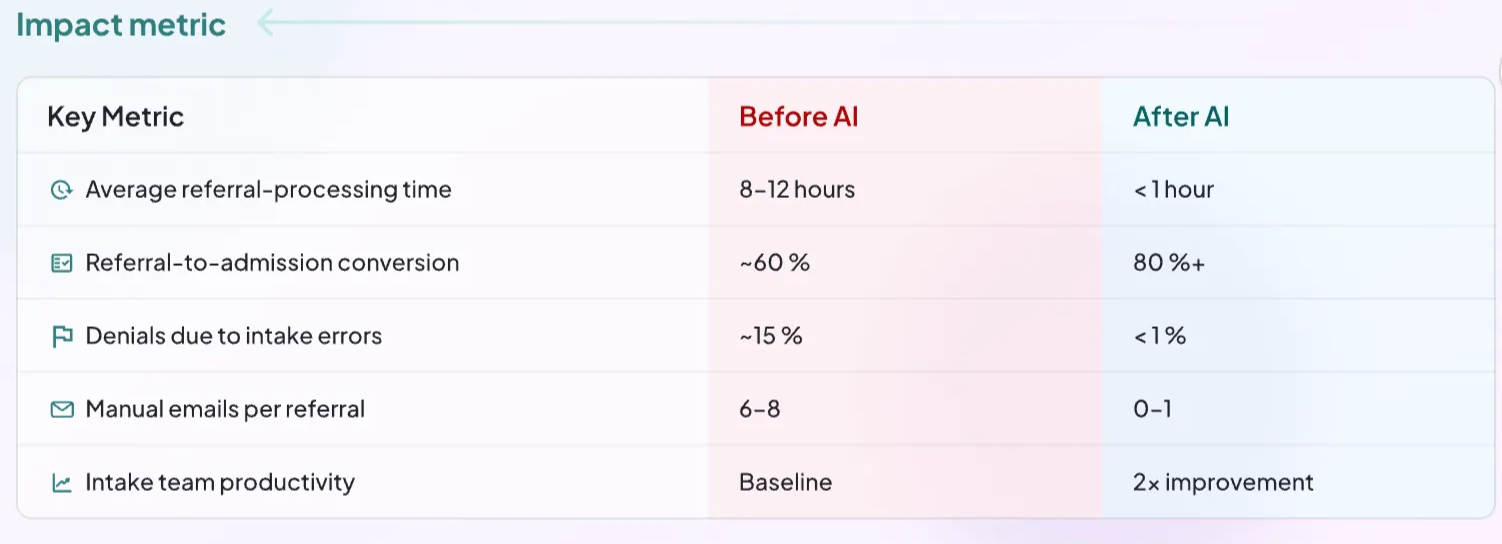
The difference isn't marginal. It's transformational.
The Value-Based Care Multiplier Effect
Here's where it gets interesting: RCM automation doesn't just improve your billing—it makes value-based contracts actually viable for post-acute providers.
Consider this scenario: You're in a Medicare Advantage contract where you're at risk for SNF readmissions. Manual processes mean you're always reactive, scrambling to understand why patients came back.
With automation:
- You have real-time data on which patients are high-risk for readmission
- Systems automatically schedule follow-up calls and monitor symptoms
- Care coordination activities are documented and billed appropriately
- Predictive analytics help optimize length of stay for both clinical and financial outcomes
Suddenly, you're not just managing risk—you're profiting from better outcomes.
My controversial opinion: Stop waiting for ‘Perfect’
The biggest mistake I see post-acute providers make is waiting for the "perfect" RCM solution. News flash: it doesn't exist.
What does exist are automation platforms that can eliminate 80% of your manual work tomorrow. Is it perfect? No. Will it transform your operations and financial performance? Absolutely.
Stop spending years evaluating vendors and start implementing solutions that work today. Your staff deserves better than drowning in paperwork while patients wait for care.
The Future is Here, just unevenly distributed
Some post-acute facilities are already living in 2030. They process referrals instantly, verify eligibility in real-time, and generate clean claims automatically. Their staff focuses on patient care instead of chasing payments.
Others are still stuck in 2005, manually posting payments and begging payers for information.
Which future do you want?
My recommendation: Act now or die slowly
If you're a post-acute care leader still relying on manual RCM processes, you have two choices:
- Implement comprehensive automation in the next 90 days
- Accept that you'll be out of business within 3 years
I know that sounds dramatic, but the math is simple: facilities with automated RCM processes have 30-40% lower operating costs, better cash flow, and happier staff. They can compete for value-based contracts while you're still figuring out why your denials are increasing.
The choice is yours, but time is running out.
Nanonets Health has built RCM automation specifically for post-acute care providers who are tired of excuses and ready for results. Our implementation takes weeks, not years, and ROI is visible within 30 days.
Stop accepting mediocrity. Your patients, staff, and bottom line deserve better.
Want to explore how RCM automation could transform your financial operations? Schedule a no-obligation consultation with our post-acute care specialists today.